Ankle ligaments
Understanding the anatomical structure of the ankle ligaments is critical to proper diagnosis and treatment. Damage to the ligamentous apparatus of the ankle joint is one of the most common traumatic reasons for visiting a doctor. Chronic pain in the ankle area is most often the result of a failure of one of the ligaments.
Ankle ligaments can be divided into 3 main groups: lateral (outer) group, deltoid ligament (inner group), tibiofibular ligament group.
The outer group of ligaments of the ankle joint.
Anterior talofibular ligament.
It is the most commonly damaged ankle ligament. Plays an important role in limiting the anterior displacement of the talus and plantar flexion of the foot. The ligament is located in close proximity to the joint capsule and is often represented by two bundles. The bundles are separated by vascular branches from the peroneal artery.
The anterior talofibular ligament originates from the anterior edge of the fibula 10 mm from its apex. In the neutral position of the foot, it is directed strictly horizontally and is attached to the body of the talus in its proximal part immediately on the border with the articular surface. The width of attachment to the talus is 6-10 mm.
With plantar flexion of the foot, the upper bundle of the tendon is loaded, with dorsiflexion, on the contrary, only the lower bundle is loaded.
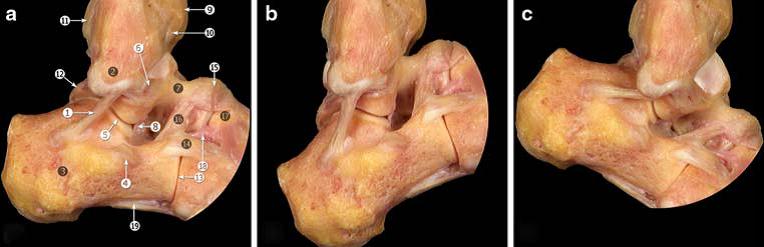
Calcaneo-fibular ligament.
It originates directly below the anterior talofibular ligament. The fibers connecting these sheaves are often found. In the neutral position of the foot, it goes down and slightly backward, heading towards its insertion on the outer surface of the calcaneus. The ligament has a round section, 6-8 mm in diameter, 20 mm long. At the same time, almost throughout its entire length, the calcaneofibular ligament is covered with tendons of the peroneal muscles.

The calcaneofibular ligament is separated from the articular capsule, but has a posterior wall of the synovial sheath of the peroneal muscles that covers it almost throughout its entire length.
In 1/3 of cases, the calcaneofibular ligament is connected to the talocalcaneal ligament. Isolated ruptures of the calcaneal-fibular ligament are extremely rare. Most often, simultaneous damage to the anterior talofibular and calcaneal-fibular ligaments occurs.
The calcaneofibular ligament remains in tension during both dorsal and plantar flexion of the foot, it relaxes in the position of the foot valgus and is most strongly strained in the position of the foot varus.
The calcaneofibular ligament assumes an almost vertical position with dorsiflexion of the foot and a horizontal position with plantar flexion of the foot.
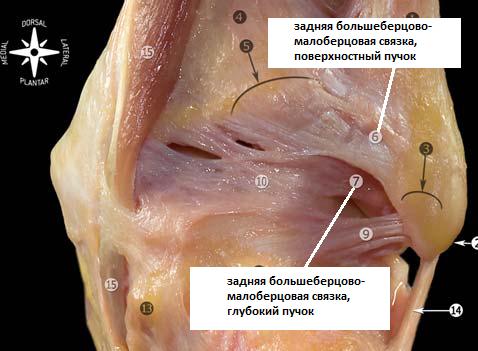
Posterior talofibular ligament.
It is located horizontally, originates from the inner surface of the fibula and is attached to the posterior outer surface of the talus. In the neutral position of the foot, the ligament is relaxed, and becomes tense when the foot is dorsiflexed.
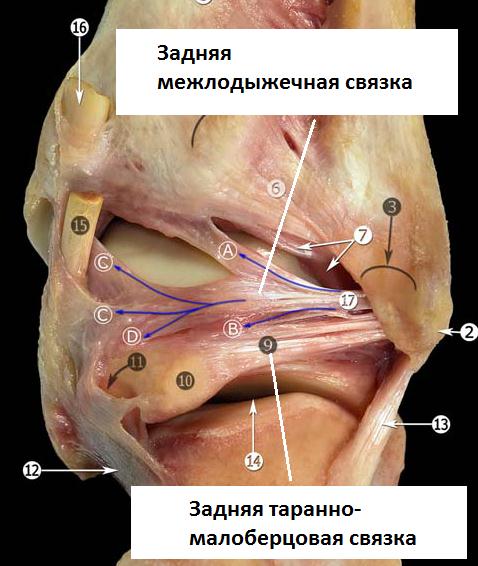
Due to its multifascicular structure, the posterior talofibular ligament is attached to the broad base along the entire posteroexternal surface of the talus, to the external process of the talus, and to the triangular bone.
In close proximity is the posterior intermalleolar (intermalleolar) ligament. Representing a thin connective tissue plate, the posterior intermalleolar ligament has a diverse anatomical structure, represented by several differently directed bundles. Like the posterior talofibular ligament, it can be damaged by forced dorsiflexion of the foot.
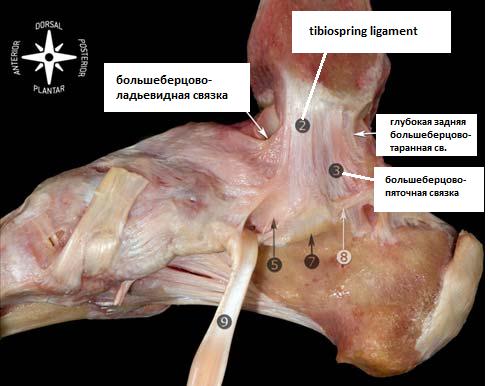
Deltoid ligament.
Most authors subdivide the medial collateral ligaments into two layers - superficial and deep. Milner and Soams distinguish the following main bundles of the deltoid ligament: Superficial layer - tibiospring, tibionavicular, deep layer - deep posterior tibio-talar ligament. And also 3 additional beams: superficial - superficial tibial-talar St., tibiocalcaneal St., anterior deep tibial-talar St. In a number of situations, it is possible to identify all six main bundles, but their location varies greatly within the anatomical norm, and some of the bundles may be completely absent in some cases. Therefore, this classification is conditional and is of scientific rather than clinical interest.
Group of ligaments of the tibiofibular joint.
The ankle joint is formed by three bones: the talus, tibia, and fibula. The tibia and fibula form a fork, or groove, within which the talar block moves. The connection of the tibia is syndesmotic and provides a certain mobility. With dorsiflexion of the foot, the tibiofibular gap expands, the fibula rises and rotates inward. In plantar flexion, on the contrary, it descends and rotates outward. The tibiofibular ligaments prevent excessive movement of the fibula outwards, backwards, anteriorly, and also limit its rotation.
Anterior-inferior tibiofibular ligament. It connects the anterolateral tubercle of the tibia (Chaput's tubercle) and the anterior tubercle of the fibula (Wagstaffe's tubercle). The posterior-inferior tibiofibular ligament connects the posterior tubercle of the tibia (Volkmann's tubercle) and the posterior aspect of the lateral malleolus. It is the most powerful component of the tibiofibular syndesmosis.
In addition to these structures located anterior and posterior to the tibia, directly between them are: the transverse tibiofibular ligament, interosseous membrane, interosseous ligament and lower transverse ligament.

The interosseous tibiofibular ligament is a multiple short rigid fibers that are essentially a continuation of the interosseous membrane. Its role in the stabilization of syndesmosis is regarded by the authors of anatomical studies in different ways. Some give it paramount importance, others believe that it does not play an important role.
Understanding the structure of the ligamentous apparatus of the ankle joint is fundamental in the diagnosis and treatment of injuries in this area. Assessment of the mechanism of injury suggests the possible development of subsequent instability or the formation of an impingement syndrome. Surgical treatment of this pathology is impossible without a clear knowledge of the topographic anatomy of the main ligamentous structures.
In preparing the article, materials from Pau Golano, anatomy of the ankle ligaments, 2010 were used.